Content 1
Content 2
Content 3
Straight lines that appear crooked
Straight lines that appear crooked
Straight lines that appear crooked
Straight lines that appear crooked
Genetics
Family history3 (genetic predisposition)
Genetics
Family history3 (genetic predisposition)
Genetics
Family history3 (genetic predisposition)
Genetics
Family history3 (genetic predisposition)
There is an FDA-approved treatment option for GA secondary to AMD
There is an FDA-approved treatment option for GA secondary to AMD
There is an FDA-approved treatment option for GA secondary to AMD
Out of 201 eyes, 75 eyes were coded as early or intermediate AMD5*
But when using the Hoover categorization
did not have GA
47%
(n=35/75)

had GA
53%
(n=40/75)
See how GA may impact your patients
Learn more about an FDA-approved treatment option for GA secondary to AMD
GA is the advanced form of dry age-related macular degeneration (AMD), and progression to GA is a frequent outcome of dry AMD.4,7-10
Click on the tabs below to learn more.
Healthy OCT B-scan
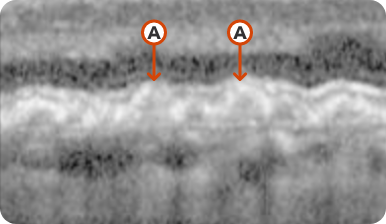
Few medium-sized drusen
Healthy OCT B-scan
Few medium-sized drusen
Hyperreflective foci representing RPE migration
Healthy OCT B-scan
Few medium-sized drusen
Healthy OCT B-scan
Few medium-sized drusen
Hyperreflective foci representing RPE migration
Images may vary based on different device manufacturers and imaging platforms.
What to look for:
Considerations:
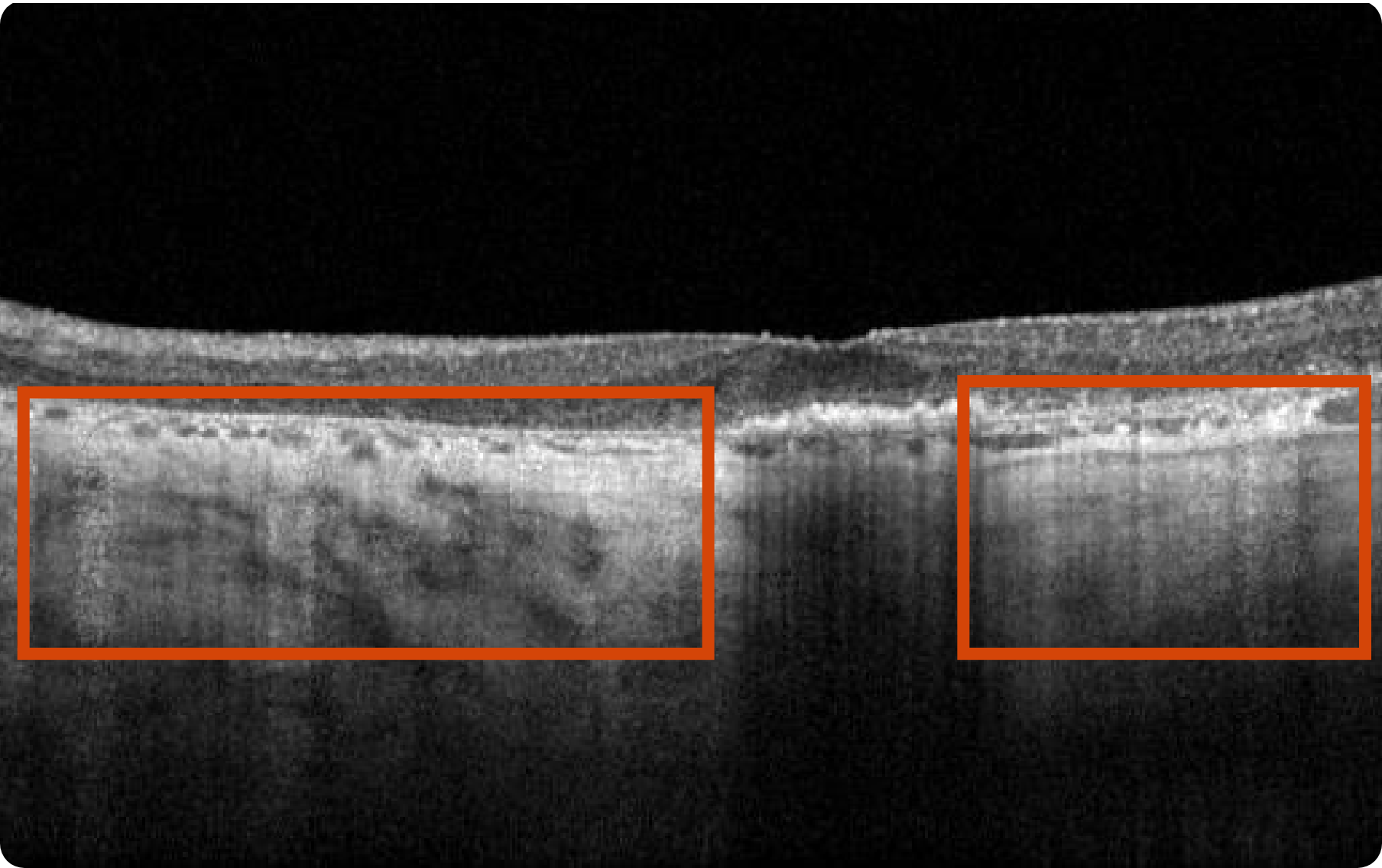
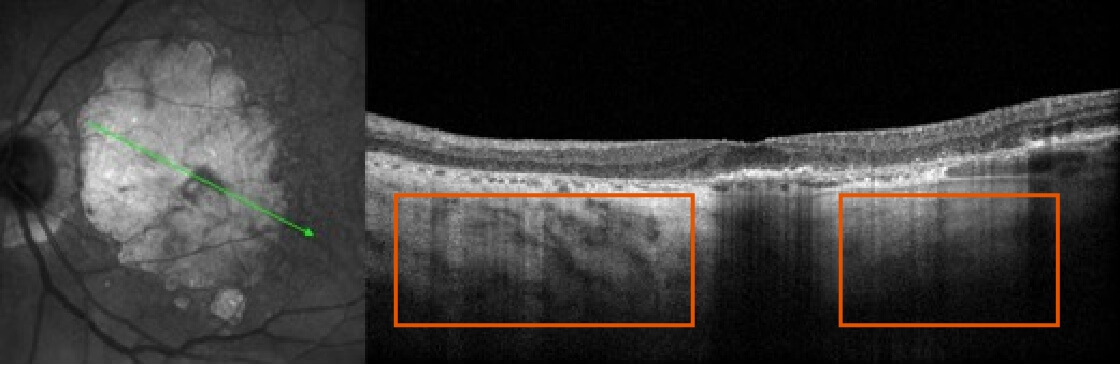
If you do not have access to FAF imaging, OCT en face can be used as a substitute to visualize the full extent of GA lesions. On certain machines, NIR images can be acquired simultaneously with OCT en face images. Using both OCT en face and NIR scans allows for the highest accuracy in detecting RPE indicative of GA.7,13
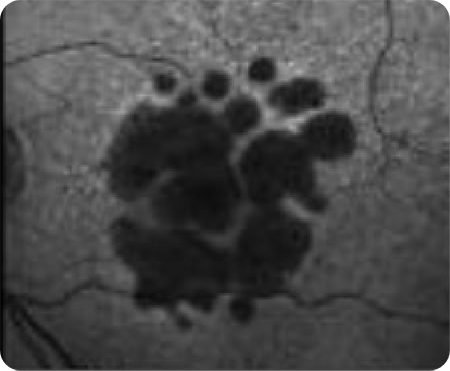
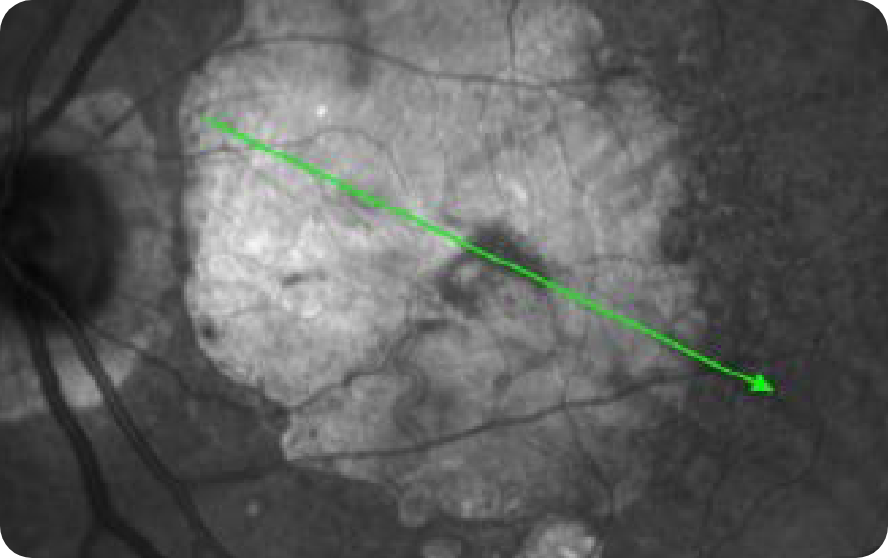
Healthy OCT en face Image*
OCT en face Image 1
Multifocal lesion appears as a bright area due to increased penetration of light into the choroid caused by RPE and outer retina atrophy14
OCT en face Image 2
Progression of larger multifocal lesion with subfoveal involvement14
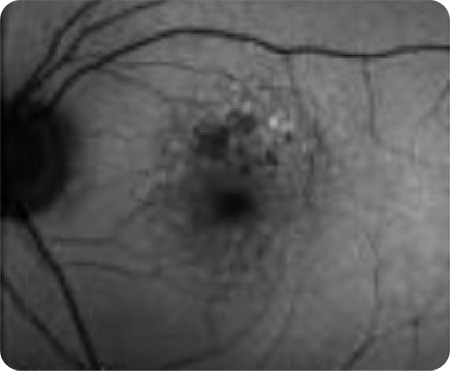
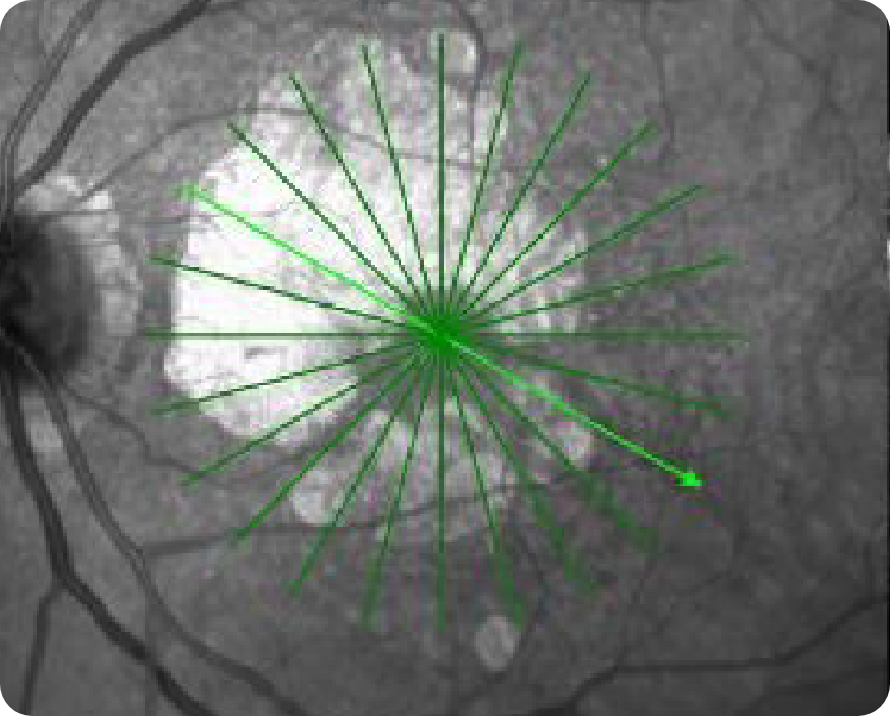
Healthy NIR Image
NIR Image 1*
Multifocal lesion appears as a bright area due to increased penetration of light into the choroid caused by RPE and outer retina atrophy14
NIR Image 2*
Multifocal lesion appears as a bright area due to increased penetration of light into the choroid caused by RPE and outer retina atrophy14
Images may vary based on different device manufacturers and imaging platforms.
Images may vary based on different device manufacturers and imaging platforms.
What to look for:
Considerations:
Healthy OCT B-scan
Few medium-sized drusen
Healthy OCT B-scan
Few medium-sized drusen
Hyperreflective foci representing RPE migration
Healthy OCT B-scan
Few medium-sized drusen
Healthy OCT B-scan
Few medium-sized drusen
Hyperreflective foci representing RPE migration
Images may vary based on different device manufacturers and imaging platforms.
What to look for:
Considerations:
Healthy OCT B-scan
Few medium-sized drusen
Healthy OCT B-scan
Few medium-sized drusen
Hyperreflective foci representing RPE migration
Healthy OCT B-scan
Few medium-sized drusen
Healthy OCT B-scan
Few medium-sized drusen
Hyperreflective foci representing RPE migration
Images may vary based on different device manufacturers and imaging platforms.
What to look for:
Considerations:
Diffuse and banded patterns are associated with a higher risk of disease progression.
Images may vary based on different device manufacturers and imaging platforms.

80-year-old woman
Hypothetical patient
Medical history:
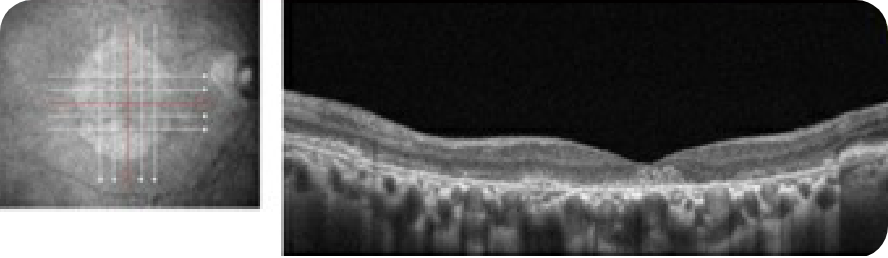
Baseline
NIR and OCT B-scan
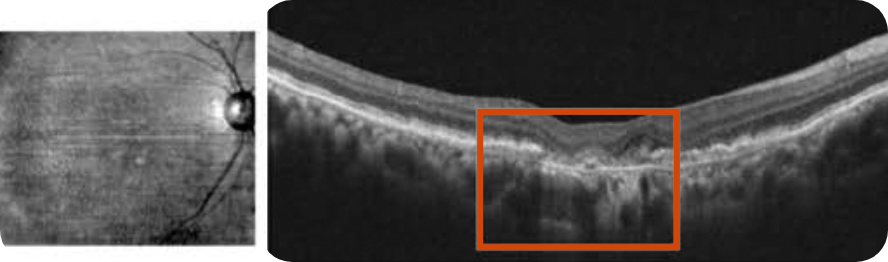
Despite significant atrophy, the fovea is still partially intact
Hypertransmission defect outside the fovea; subsidence of OPL and INL can be seen around the area of atrophy
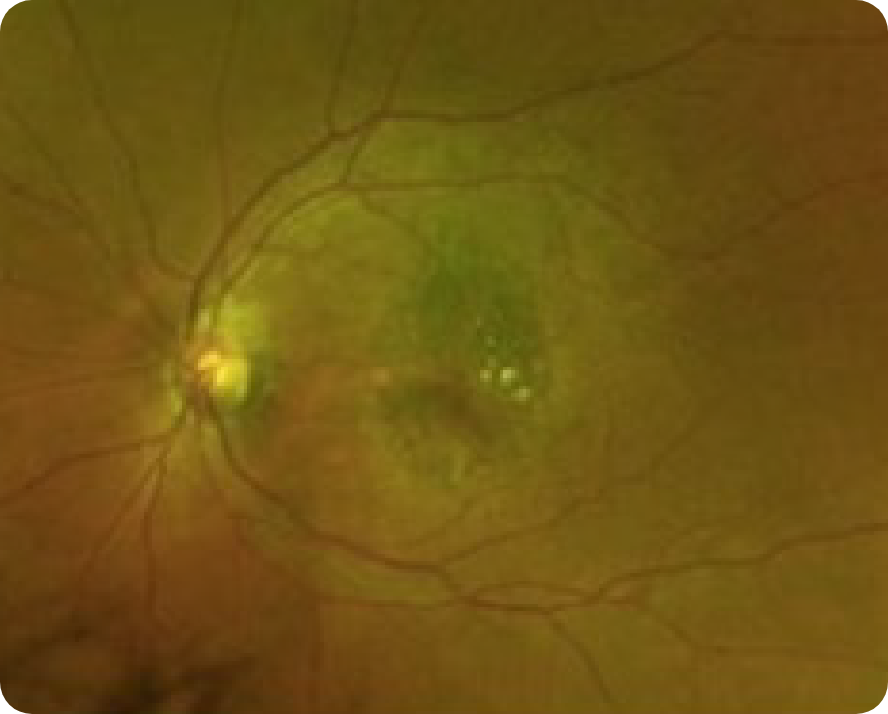
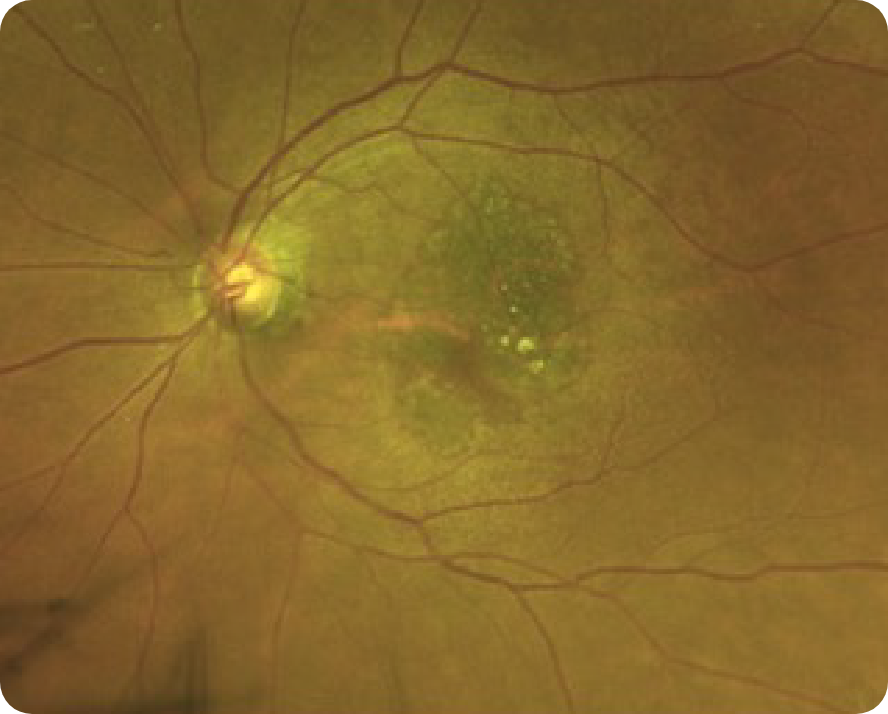
CFP
2 Years After (2020)
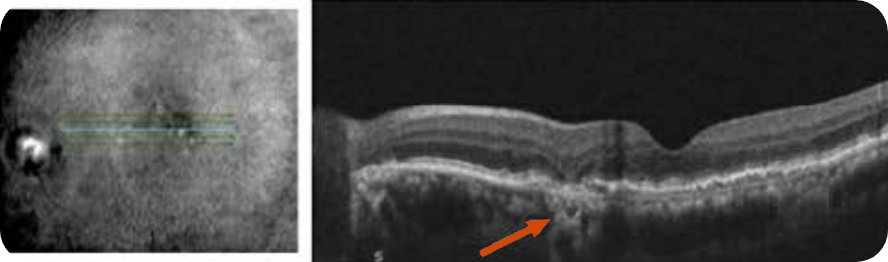
OCT B-scan and en face
Complete RPE and outer retinal atrophy (cRORA) parafoveally
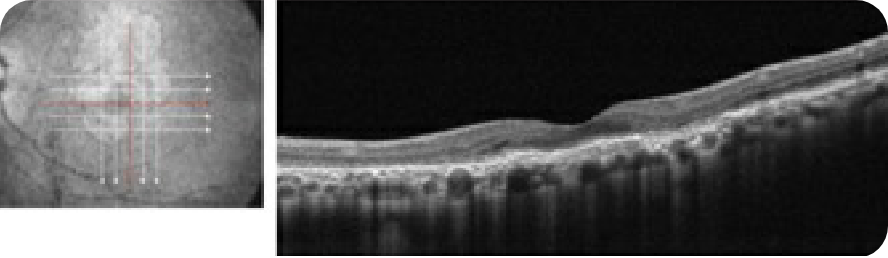
cRORA with choroidal hypertransmission defect. Visual acuity is still somewhat preserved due to partial foveal sparing
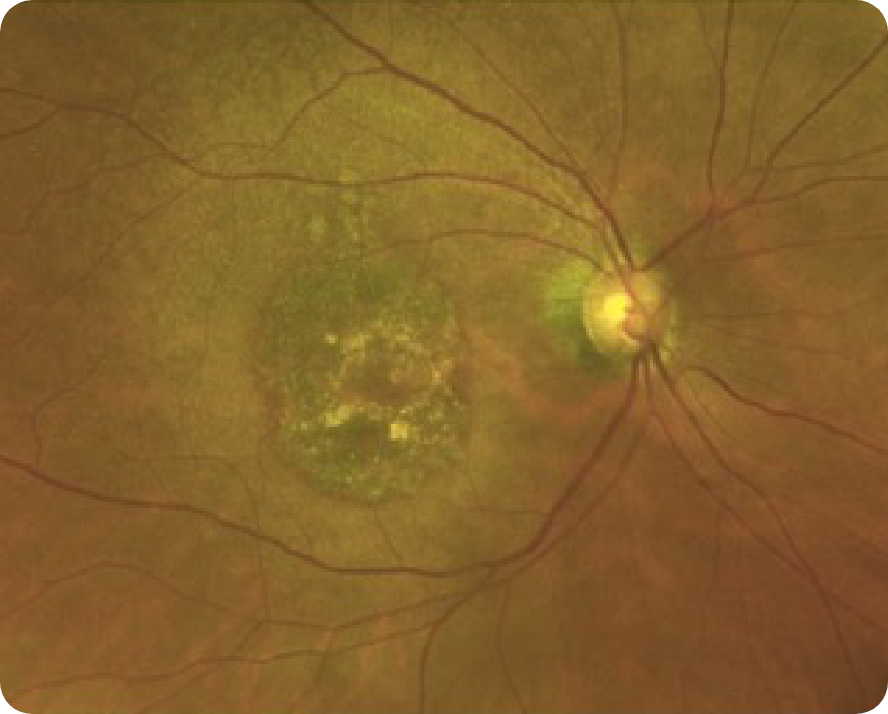
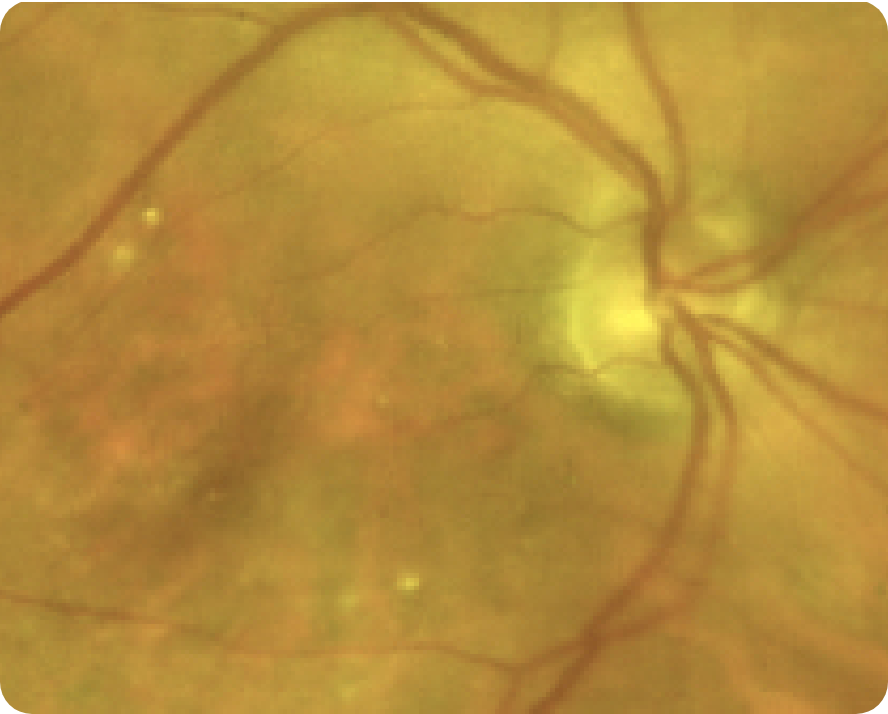
CFP
Images may vary based on different device manufacturers and imaging platforms.
71-year-old man
Hypothetical patient
Medical history:
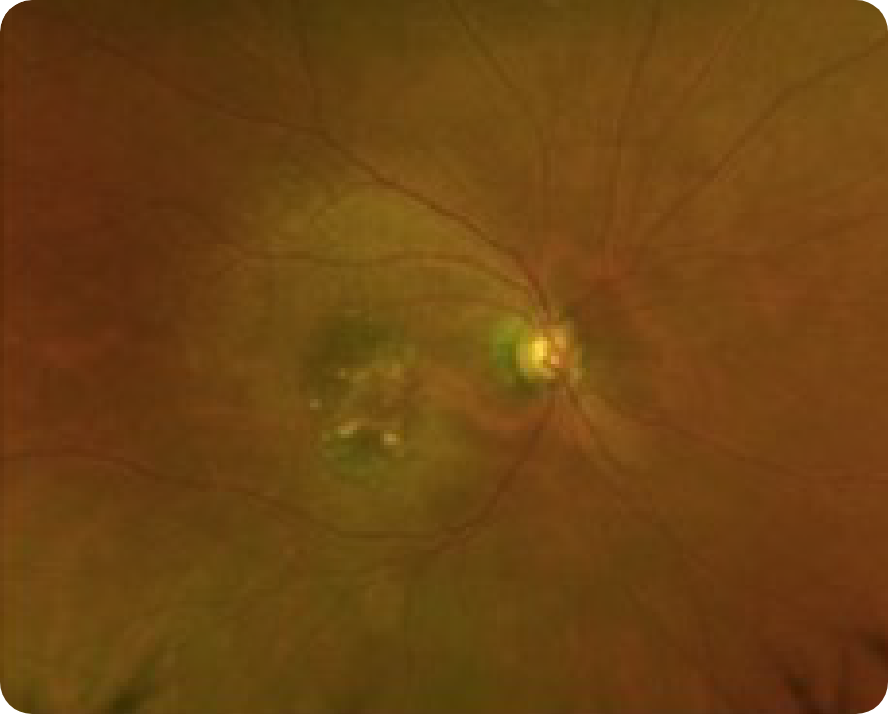
CFP

Shows some area of GA
GA is less apparent
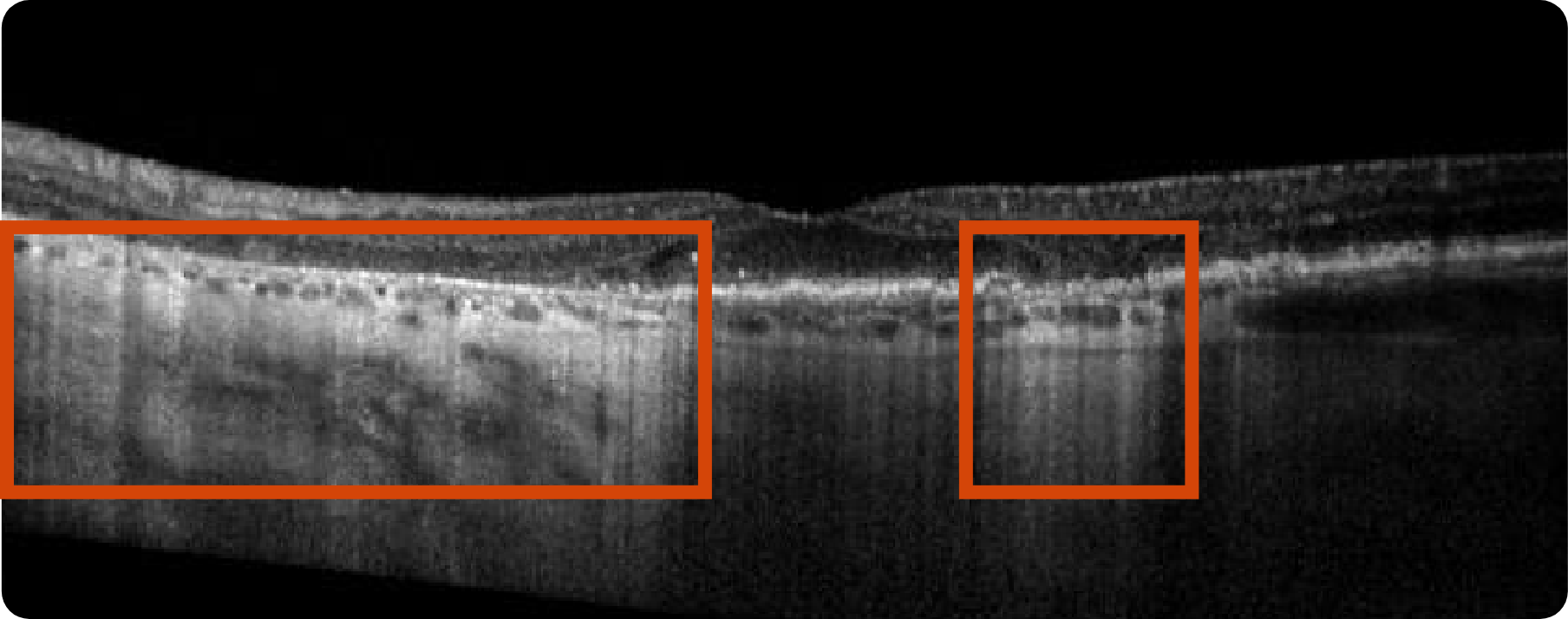
OCT B-scan
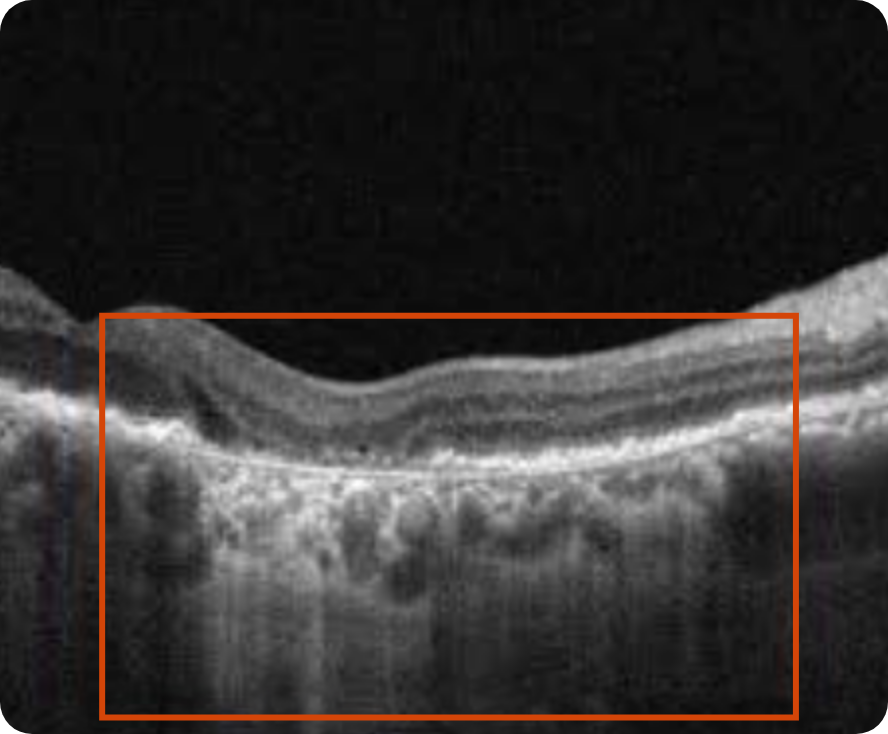
Complete RPE and outer retinal atrophy (cRORA) with increased hypertransmission into choroid
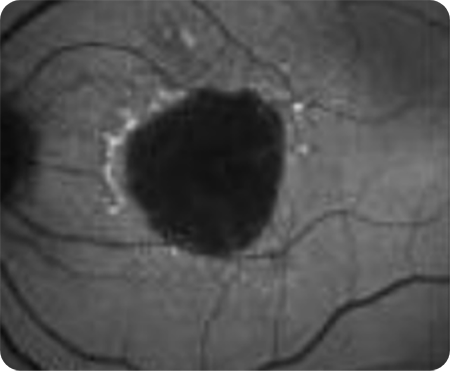
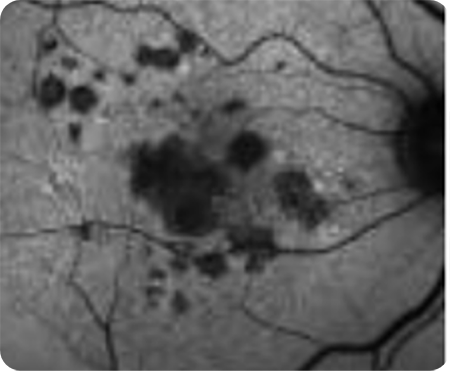
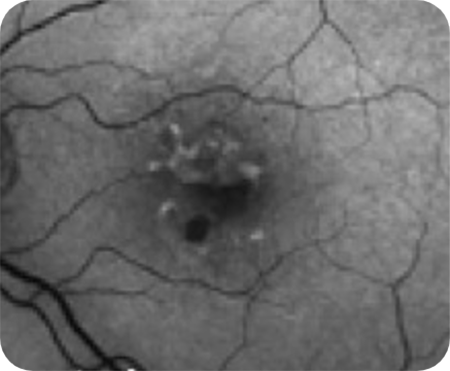
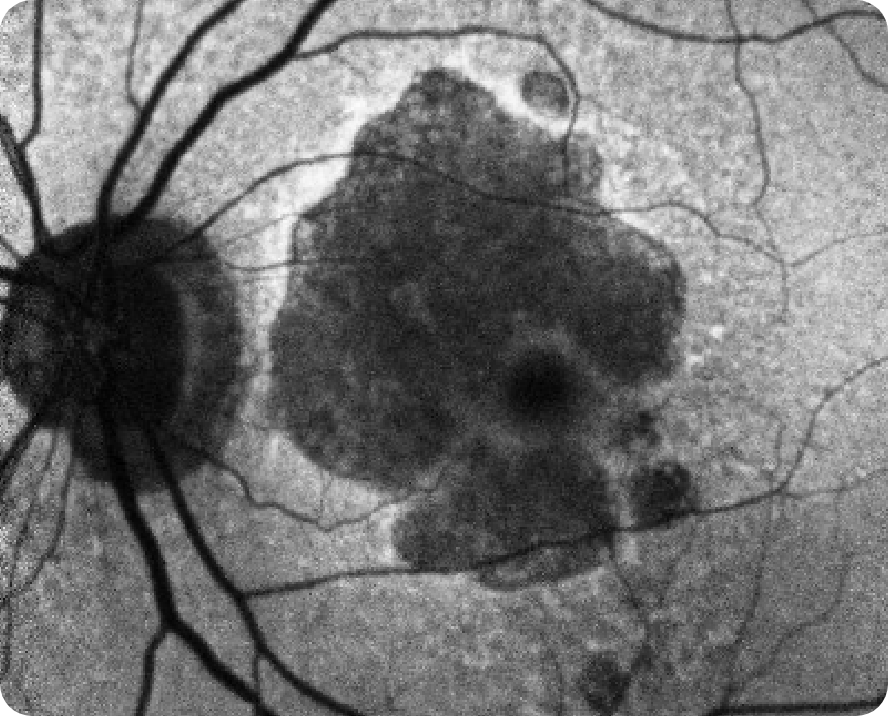
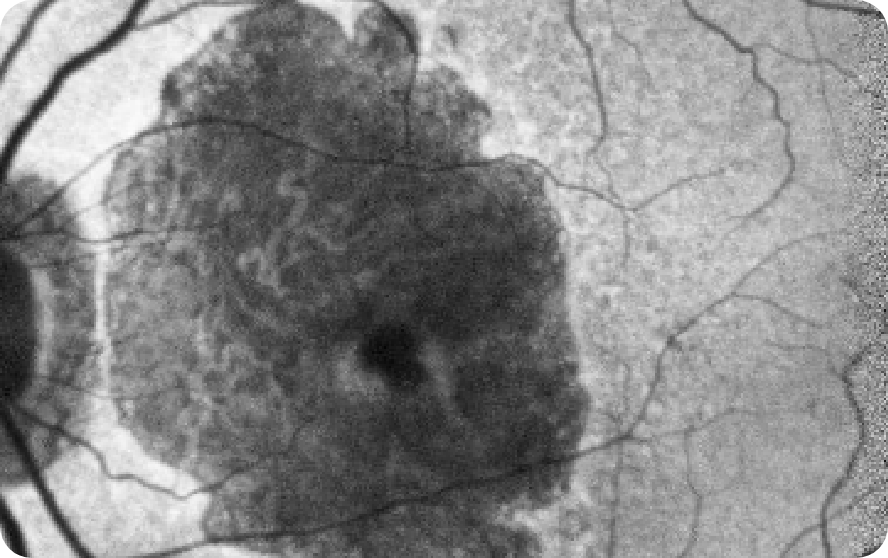
FAF

Lesion without subfoveal involvement; hyperfluorescent border around the GA lesions indicating areas that are at risk for further progression
Images may vary based on different device manufacturers and imaging platforms.
80-year-old woman
Hypothetical patient
Medical history:
Baseline
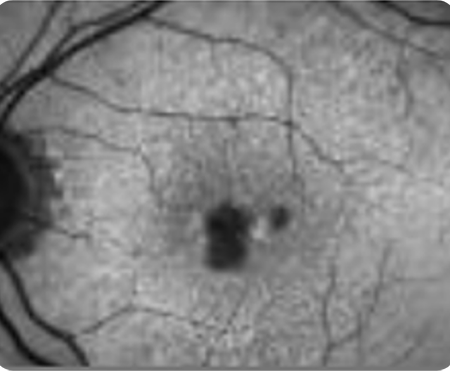
FAF
Despite significant atrophy, the fovea is still partially intact
NIR
CFP
Significant atrophy outside the fovea as shown by choroidal hypertransmission defect
4 Years After
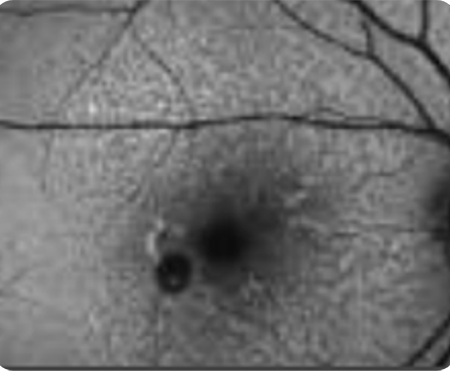
FAF OS
NIR OS
OCT OS
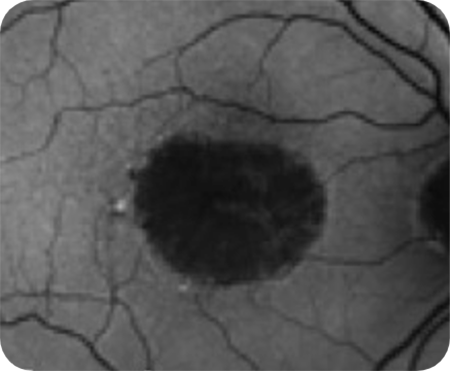
Area of atrophy has grown, as shown by larger region of choroidal hypertransmission. The fovea still remains relatively spared
Images courtesy of Mohammad Rafieetary, OD, Charles Retina Institute.
See how GA may impact your patients
OCT header image courtesy of Dr Julie Rodman, OD, Broward Eye Care Institute.
AMD=age-related macular degeneration; BCVA=best-corrected visual acuity; OCT=optical coherence tomography; RPE=retinal pigment epithelium.
*Baseline and Year 4 images courtesy of Dr Mohammad Rafieetary, OD, Charles Retina Institute.
†The Age-related Eye Disease Study (AREDS) #26, a long-term, multicenter, prospective study examining the progression of GA area in a cohort of 3640 patients with signs of early and more advanced forms of AMD.3
‡The global Geographic Atrophy Insights Survey (GAINS) was sponsored by Apellis and conducted by The Harris Poll between October 12 to December 10, 2021. To accommodate visually impaired respondents, the survey was conducted online and via the telephone among 203 participants aged 60 or over (mean age 70 years) residing in the US, UK, France, Germany, Italy, Netherlands, Sweden, Canada, and Australia who self-reported that they have been diagnosed with age-related macular degeneration (AMD) and have dry AMD in at least one of their eyes. They must also have indicated that they have advanced atrophic age-related macular degeneration or advanced atrophic AMD, advanced/late/late-stage dry age-related macular degeneration or advanced dry AMD, or geographic atrophy (GA) in one or both of their eyes. Included patients must have been currently experiencing at least 3 GA symptoms and currently do/used to do/or have been suggested by an eye care professional but have not done at least one of the following: Take a high-dose formulation of antioxidant vitamins and minerals, stop smoking, maintain a healthy weight and exercise regularly, choose a healthy diet, manage other medical conditions, have check-ups of the retina regularly, or wear sunglasses with UV protection. Included patients must not have been diagnosed with glaucoma, Stargardt disease, or dementia, or be receiving regular injections into the affected eye every 4 to 6 weeks.11
Year 4
BCVA: 20/25
Choroidal hypertransmission defect indicative of atrophy.
You are now leaving RecognizeAndReferGA.com
This link will take you to another Apellis Pharmaceuticals, Inc. website.
Are you a US eye care professional?